After the Official Journal harmonised EN 60601-1 on 17 June 2026, I later wrote up an overview: what changed, the nine-year wait, what to cite, and the EC REP to EU REP switch riding alongside it. Then the comments started, and the good ones went straight past the headline. This is the deeper cut.
This post assumes you already know that EN 60601-1:2006/A13:2024 landed at entry No. 65 and that A13 carries Annex ZZ. From here I want to answer the questions my readers actually asked. I have deliberately not repeated much of what is already in the LinkedIn article, which covers the background, the full decision, and several points I do not revisit here, so it is worth reading alongside this.
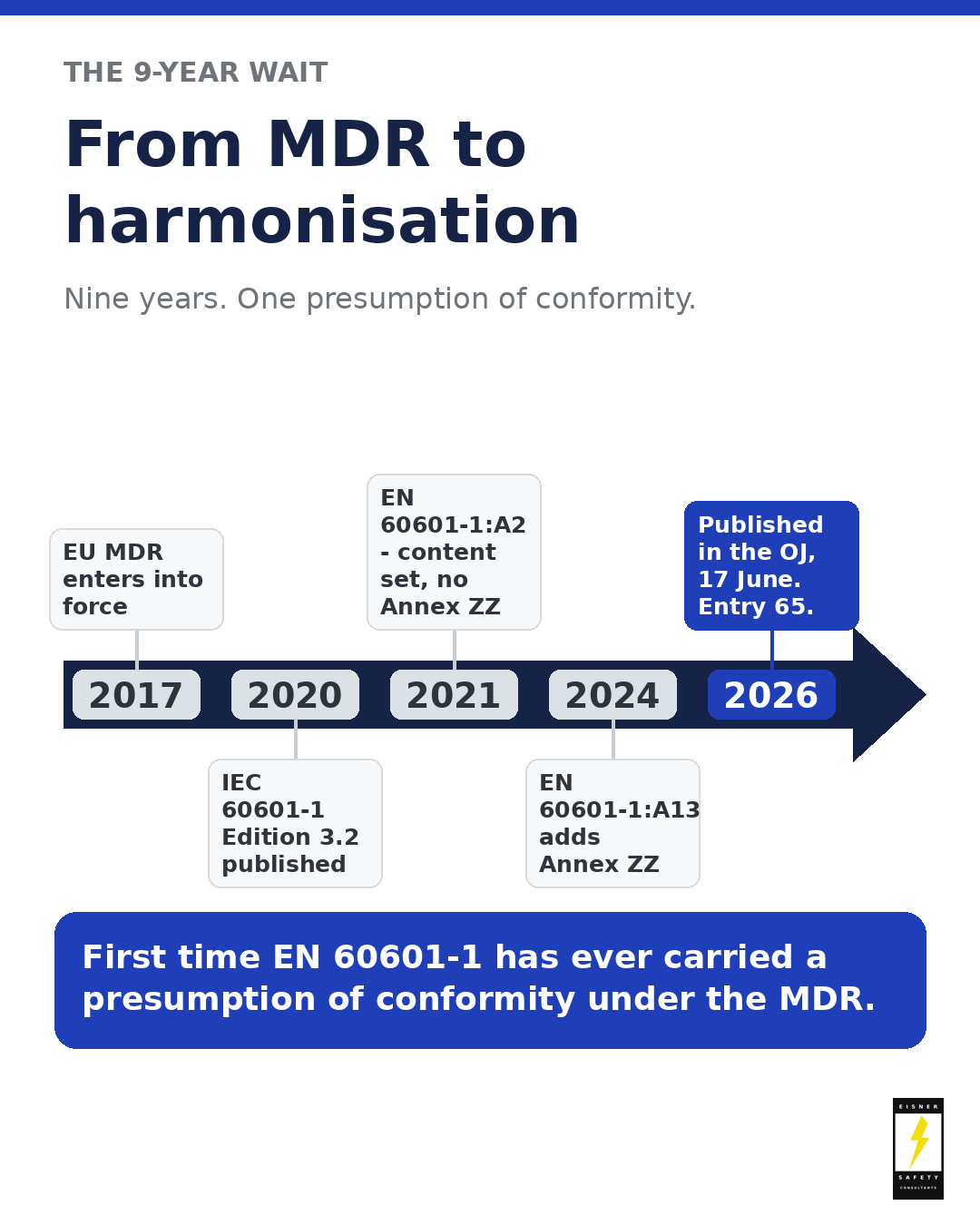
The nine-year road from the MDR to entry 65.
Resources for this post
- Download the one-page cheat-sheet (PDF)
- Read the LinkedIn article
- See the LinkedIn launch post & comments
- Join the newsletter
- Schedule a call with Leo, “the IEC 60601 Guy”
What a presumption of conformity really buys you
Here is the sentence people skip: a harmonised standard gives you a presumption of conformity only for the requirements Annex ZZ says it covers. Not the whole of Annex I. Not “the device is compliant.” Just the specific General Safety and Performance Requirements (GSPRs) the table maps.
Annex ZZ is formally informative. It was prepared under mandate M/575 as one voluntary means of conforming, and it spells out the mechanism: once the standard is cited in the Official Journal, compliance with the normative clauses in its Table ZZ.1 confers a presumption of conformity, but only within the scope of the standard.
Look at Table ZZ.1 itself, the mapping table inside Annex ZZ, and its limits jump out. In its “Remarks / Notes” column, coverage is stated again and again as basic safety and essential performance within the scope of the EN, not the whole of a requirement. Whole categories come back “not covered” or only “partly covered,” because 60601-1 addresses them only by pointing to other standards: biocompatibility, EMC, usability, and sterilization all fall into that bucket. The standard says so in its own notes: if a GSPR is not in Table ZZ.1, it is not addressed here.
Annex ZZ also carries Table ZZ.2, the terms where the MDR definition prevails over the standard’s. “Harm” in the standard reaches property and the environment; under the MDR it narrows to people. “Patient” means human use only under the MDR, whereas in the EN it has always included animals and will continue to do so in the 4th edition. “Risk management” as the MDR uses it is broader, so the standard’s coverage of it is correspondingly limited. A reviewer reads your file against the regulation’s vocabulary, not the standard’s.
So the real work is not “we cite the harmonised standard, therefore we are covered.” Run it as a gap analysis: lay every Annex I GSPR as a row; for each one Annex ZZ maps, record the clause and copy any partial-coverage qualifier word for word; for the GSPRs 60601-1 does not touch (biocompatibility, EMC, sterilization, much of usability, clinical, labelling content), name the other standard, test, or risk-file evidence that carries it; and flag anything leaning on an older or non-harmonised source before a reviewer does.
Two Z-annexes, two different jobs: do not confuse ZA with ZZ
While everyone talks about Annex ZZ, do not walk past Annex ZA. They look alike and do completely different things.
Annex ZZ (informative by designation, but the mechanism the Official Journal citation activates) maps the standard’s clauses to the MDR GSPRs and supports the presumption of conformity. Annex ZA is the normative references table: it lists every IEC and ISO publication the standard depends on and gives the corresponding European (EN/HD) version. Being normative, those references are part of the requirements.
Annex ZA carries two rules that quietly decide what you must meet. First, dated versus undated references: for a dated reference only the cited edition applies; for an undated one the latest edition, including amendments, applies, so it moves under your feet over time. Second, “(mod)” means the international text was changed by European common modifications and the EN/HD applies, not the plain IEC or ISO version.
The Z-annexes for the EN 60601 and EN 80601 series standards are drafted by CENELEC, in TC 62 WG 2 for medical devices. The members of that committee have written a guide titled the “Cookbook” for writing harmonised standards under the MDR and IVDR. Beat Keller, one of my ESC experts, is a member of that committee. The cookbook exists to give the writers of these harmonised European standards practical, consistent ways to handle the European forewords and the Z-annexes, and in particular to resolve the issues raised during HAS consultant assessments of draft standards. It is not a minor internal note either: the European Commission’s DG SANTE and the MDCG standards subgroup judged its first edition “in principle complete and ready for use” back in November 2022, which made it a solid basis for writing the harmonised standards in this series and their annexes.
“Harmonised” is not the same as “state of the art”
One of the sharpest points from the comments is worth making loudly: presumption of conformity and state of the art are two different tests, and passing one does not pass the other.
A harmonised standard, applied in scope, gives presumption of conformity for the GSPRs it covers. State of the art is a separate expectation running through the MDR’s GSPRs in Annex I, and it is not defined in the regulation. In practice the newest recognised edition is treated as the state of the art, even when that edition is not the harmonised one. So the version that gives you the presumption can be older than the version that represents the state of the art, and when they diverge you can be presumed conformant and still be expected to show how you meet the current state of the art.
A concrete example sits inside this very decision. Before 17 June 2026, citing the older EN ISO 10993-23:2021 held a valid presumption, yet its 2025 amendment was already the newer state of the art. The same Decision (EU) 2026/1231 then harmonised the amended versions and set the old ones to be withdrawn from 15 December 2027. That lag is the normal rhythm, not a glitch: when a newer edition appears, assess it as potential state of the art even while you still cite the harmonised version for presumption.
And the citation question that came up in the comments now has a clear answer. For use under the MDR, cite the full amendment chain: EN 60601-1:2006+A1:2013+A12:2014+A2:2021+A13:2024, which corresponds to IEC 60601-1:2005+A1:2012+A2:2020 (Edition 3.2, with A13:2024 carrying Annex ZZ). That is how the standard designates itself on its own cover, and it is what belongs on your Declaration of Conformity and standards list. The clipped “EN 60601-1:2006/A13:2024” is fine for a headline, not for your technical documentation.
Legacy devices and the audit question
Now that 60601-1 is harmonised, will Notified Bodies scrutinise how legacy data lines up with it? First the framework. Legacy devices on valid MDD or AIMDD certificates under Article 120(3) of the MDR, as amended by Regulation (EU) 2023/607, may stay on the market to the 2027 or 2028 dates provided they keep conforming to their directive and undergo no significant change (MDCG 2020-3). They are not required to re-certify to a harmonised 60601-1. What continues to apply are the ongoing MDR obligations, including post-market surveillance, vigilance, and risk management.
So the new listing does not, by itself, force anything onto a legacy device. But once a current harmonised reference exists, it becomes the obvious yardstick, and reviewers reach for the obvious yardstick. For devices in MDR conformity assessment now, EN 60601-1:2006/A13:2024 is the reference to build against; for legacy devices, expect questions less about re-certifying and more about whether your risk management and post-market data still hold up against the current state of the art. Depending on what your risk management and any gap assessment turn up, that can, in some cases, push you toward a more current version of the standard.
The scope trap: your medical device might also be “machinery”
Here is one that quietly catches manufacturers, buried in the same Annex ZZ. Under Article 1(12) of the MDR, a medical device can also be machinery within the meaning of the EU Machinery Directive (2006/42/EC). When it is, certain Essential Health and Safety Requirements of that directive that are more specific than the MDR GSPRs apply on top of the MDR, and the standard maps them in Table ZZ.3.
In practice this bites devices with lifting parts or accessible non-manual moving parts: patient hoists, powered tables and chairs, motorised carriers. Two things people get wrong. First, Table ZZ.3 does not give you a presumption of conformity under the Machinery Directive and implies no Official Journal citation under it; it only maps where the machinery requirements are more specific. Second, the Machinery Directive is on its way out: Regulation (EU) 2023/1230 replaces it from 20 January 2027, so plan against the new Machinery Regulation, not the old Directive.
This is one of the most commonly missed corners of 60601-1 compliance, and untangling it is exactly the kind of scope work my team does. If your device lifts, rolls, or has powered moving parts an operator can reach, do not assume the MDR is the whole story.
Why “EC REP” existed in the first place
“EC” stands for European Community, the correct legal name until the Treaty of Lisbon replaced it with “European Union” in December 2009. So the “EC” in “EC REP” has been out of step with the Union’s own vocabulary for more than fifteen years. That is the whole reason for the move to “EU REP,” and it is why MDCG 2021-5 Rev. 1 can call it “purely editorial.” The generic symbol itself comes from EN ISO 15223-1: the standard defines an “XX REP” where “XX” is the ISO 3166-1 country code, and the Commission worked with the ISO working group to land on “EU” for the Union. The change did not appear from nowhere. It began as Amendment 2 to standardisation request M/575 (Commission decision C(2024)3371) in May 2024, when the Commission asked CEN and CENELEC to introduce “EU REP” and drop any reference to “European Community.” CEN and CENELEC accepted, ISO adopted the amendment, the EN amendment followed, and the reference was published in the Official Journal on 17 June 2026, harmonised under both the MDR (Decision (EU) 2026/1231) and the IVDR (Decision (EU) 2026/1313). So this is not a rename someone slipped in; it is a deliberate, traceable alignment of the symbol with the Union’s own legal language.
The change is editorial. The change control around it is not free.
The symbol change needs no prior Notified Body approval on its own, and you have five years of coexistence. All true. But “no approval needed” is not “free.” Labelling changes cost money and time no matter how small the wording, so most manufacturers batch the swap into the next artwork refresh. That is where the “editorial” framing bites: the moment you bundle EU REP with any change that is not editorial, you can pull the whole batch into Notified Body territory. Treat the five-year window as planning room, look at everything else riding in the cycle, and use the same pass to retire other “European Community” era wording, including any lingering “EC Declaration of Conformity.” It also helps to know how much room the MDCG actually gives you. During the five-year window both symbols are valid, and you may even carry “EC REP” and “EU REP” on different levels of the same packaging, with re-labelling or over-labelling accepted, as long as the authorised-representative information stays clear. Devices already on the market with “EC REP” before the deadline can continue to be made available. One date to put in your plan: the MDCG appendix and the IVDR decision give the end date as 17 June 2031, but the binding MDR text (Article 2 of Decision (EU) 2026/1231) deletes the old reference from 15 June 2031, two days earlier, so cite the binding date in your technical documentation.
The signal I care about most
Look past the individual entries and there is a bigger story. The harmonisation route for medical electrical standards had been stuck for years, and this decision is evidence that it is moving again. For those of us working on the IEC 60601-1, 4th edition, and the future of the series, that matters more than any single listing: a new edition is only as useful as its route to recognition. Entry 65 is one line in the Official Journal, but it tells me the door is open again.
The bottom line
Entry 65 was the easy part. The harder, more useful work is downstream: reading Annex ZZ for what it actually covers, holding presumption of conformity and state of the art as two separate tests, keeping legacy devices honest against a sharper yardstick, catching the machinery scope trap, and treating the “editorial” label change as a change-control decision. None of that fits in a post. That is why it lives here. And because this piece deliberately does not rehash the LinkedIn article, go back to it for the full decision and the details I did not repeat here.
Download the one-page cheat-sheet (PDF): entry 65, what to cite now, the EU REP dates, and official EU sources in one place.
Turn this into practical action
My team and I at Eisner Safety Consultants work with medical device, IVD, and combination product manufacturers to turn standards into practical design inputs, GSPR and gap analysis, labelling, test strategy, and technical documentation. That includes the machinery-scope questions many teams miss, and it is the kind of work we do every day. If any of this maps onto what your team is wrestling with, I would be glad to talk it through.
About Eisner Safety Consultants
Led by Leo Eisner, “The IEC 60601 Guy,” Eisner Safety Consultants helps medtech, IVD, and combination product companies design for and demonstrate compliance to the IEC 60601 and IEC 61010 series and, for drug-device combination products, ISO 11608 needle-based injection systems. We support design reviews, identification of applicable standards and regulations, GSPR and gap analysis, labelling reviews, and test-lab and regulatory strategy. See more about our team of experts at eisnersafety.com.
Keep the conversation going on LinkedIn
- Read the full LinkedIn article: EN 60601-1 finally harmonised, and EN ISO 15223-1 ushers in “EU REP”.
- See the LinkedIn launch post & comments: “Entry 65: The Last Line,” the announcement that kicked this off.
Reference materials (official EU sources)
- Commission Implementing Decision (EU) 2026/1231 (MDR)
- Commission Implementing Decision (EU) 2026/1313 (IVDR)
- Regulation (EU) 2017/745 (MDR), Article 8, Annex I, Article 120(3)
- Regulation (EU) 2023/607 (Article 120 transitional periods)
- Regulation (EU) 2023/1230 on machinery (replaces Directive 2006/42/EC from 20 Jan 2027)
- MDCG 2020-3 Rev. 1: significant changes under Article 120
- MDCG 2021-5 Rev. 1 Appendix: transition to the ‘EU REP’ symbol